|
Overview
Pronation is the way the foot rolls inward when you walk and run. It is part of the natural movement that helps the lower leg deal with shock. Some people pronate more (overpronation) or less (underpronation) than others. Though this is not bad in itself, it does affect the way you run and it may increase the likelihood of injury. This makes your pronation pattern an important factor in choosing the right shoes. 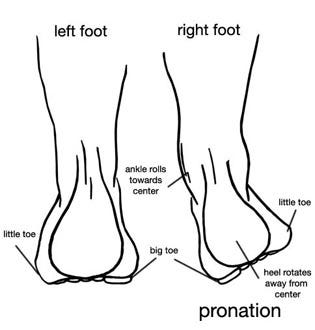 Causes In adults, the most common reason for the onset of Over-Pronation is a condition known as Post Tibial Tendonitis. This condition develops from repetitive stress on the main supporting tendon (Posterior Tibial Tendon) of the foot arch. As the body ages, ligaments and muscles can weaken. When this occurs the job of providing the majority of the support required by the foot arch is placed upon this tendon. Unfortunately, this tendon cannot bear the weight of this burden for too long. Eventually it fatigues under the added strain and in doing so the foot arch becomes progressively lower over a period of time. Symptoms When standing, your heels lean inward. When standing, one or both of your knee caps turn inward. Conditions such as a flat feet or bunions may occur. You develop knee pain when you are active or involved in athletics. The knee pain slowly goes away when you rest. You abnormally wear out the soles and heels of your shoes very quickly. Diagnosis If you have flat feet or low arches, chances are you overpronate. Although not always the case, the lower your arches the greater the overpronate. Stand on a hard surface (in front of a mirror if you need to) and look at your feet, flat feet or low arches are easy to spot. If your feet look flatter than a pancake, have a look at your ankles and see if they seem collapsed or straight. If they are, you're overpronating.  Non Surgical Treatment Overpronation is a condition in which the foot rolls excessively down and inward. The arch may elongate and collapse (or ?fall?) and the heel will lean inward. Overpronation should not be confused with pronation. Pronation is a normal motion of the foot during weight bearing and allows the foot to absorb shock as it contacts the ground. Surgical Treatment Subtalar Arthroereisis. The ankle and hindfoot bones/midfoot bones around the joint are fused, locking the bones in place and preventing all joint motion. This may also be done in combination with fusion at other joints. This is a very aggressive option usually reserved for extreme cases where no joint flexibility is present and/or the patient has severe arthritic changes in the joint. Overview
Sever disease refers to a calcaneal apophysitis (an inflammation of the apophysis of the heel) which occurs in children and young adolescents. It typically presents in active young children (especially ones who engage in jumping and running sports). Causes Sever's Disease is a repetitive strain injury caused by the following. High impact injury activities and sport like netball, football, soccer, hockey, basketball, running, jumping and tennis. Tight calf muscles. Poor mechanics, structure and function of the foot. Excessive pronation. Rapid growth spurt. The above causes tension, inflammation and pain where the Achilles tendon inserts onto the calcaneus (Back/bottom surface of the heel bone). It is important that this problem is treated and monitored until the growth plate ossifies in the heel. This could occur between the ages of 14 and 16 years of age. In extreme cases the growth plate can become separated from the calcaneus. Symptoms Pain symptoms usually begin after a child begins a new sport or sporting season, and can worsen with athletic activities that involve running and jumping. It is common for a child with Sever?s disease to walk with a limp. Increased activity can lead to heel cord tightness (Achilles Tendon), resulting in pressure on the apophysis of the calcaneus. This will cause irritation of the growth plate and sometimes swelling in the heel area thus producing pain. This usually occurs in the early stages of puberty. Diagnosis A Podiatrist can easily evaluate your child?s feet, to identify if a problem exists. Through testing the muscular flexibility. If there is a problem, a treatment plan can be create to address the issue. At the initial treatment to control movement or to support the area we may use temporary padding and strapping and depending on how successful the treatment is, a long-term treatment plan will be arranged. This long-term treatment plan may or may not involve heel raises, foot supports, muscle strengthening and or stretching. Non Surgical Treatment The following are different treatment options Rest and modify activity. Limit running and high-impact activity to rest the heel and lessen the pain. Choose one running or jumping sport to play at a time. Substitute low-impact cross-training activities to maintain cardiovascular fitness. This can include biking, swimming, using a stair-climber or elliptical machine, rowing, or inline skating. Reduce inflammation. Ice for at least 20 minutes after activity or when pain increases. Nonsteroidal anti-inflammatory drugs (NSAIDs) may also help. Stretch the calf. Increase calf flexibility by doing calf stretches for 30 to 45 seconds several times per day. Protect the heel. The shoe may need to be modified to provide the proper heel lift or arch support. Select a shoe with good arch support and heel lift if possible. Try heel lifts or heel cups in sports shoes, especially cleats. Try arch support in cleats if flat feet contribute to the problem. Take it one step at a time. Gradually resume running and impact activities as symptoms allow. Sever?s disease usually goes away when the growth plate (apophysis) matures, which should be by age 12 to 13 years in females and 13 to 14 years in males. Surgical Treatment The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Overview
 The Achilles tendon is situated above the heel and forms the lower part of the calf muscles. It is a continuation of the two calf muscles, the gastrocnemius and soleus muscles, and it attaches to the heel bone. It is the strongest tendon in the human body and must withstand great forces. Its function is to transmit the force produced by the calf muscles to lift the heel and produce the push off during walking, running and jumping. The Achilles can produce force of up to seven times body weight. This shows just how much force it has to withstand during sporting activities, such as sprinting, jumping and turning. The Achilles tendon is situated above the heel and forms the lower part of the calf muscles. It is a continuation of the two calf muscles, the gastrocnemius and soleus muscles, and it attaches to the heel bone. It is the strongest tendon in the human body and must withstand great forces. Its function is to transmit the force produced by the calf muscles to lift the heel and produce the push off during walking, running and jumping. The Achilles can produce force of up to seven times body weight. This shows just how much force it has to withstand during sporting activities, such as sprinting, jumping and turning.Causes Causes of and contributors to Achilles tendon rupture include trauma (caused by injury, usually an acceleration injury such as pushing off or jumping up). Preceding tendon problems. Chronic Achilles tendonitis (can lead to small tears within the tendon, increasingly weakening it). Certain drug therapies/treatments. Drugs that have been linked to Achilles tendon rupture include. Fluoroquinolone antibiotics - after nearly 900 reports of tendon ruptures, tendonitis and other tendon disorders (most associated with the Achilles tendon) linked to Ciprofloxacin (Cipro) alone were collected in the U.S. Food and Drug Administration (FDA)?s database, at least one public-interest group petitioned the FDA to recommend that a "Black Box Warning" be added to Cipro's packaging. Some researchers speculate this class of antibiotics is toxic to tendon fibers, and that in some cases may reduce their blood supply. Patients should at least be more aware of the potential for ruptures so that they can be switched to other antibiotics at the onset of early warning signals such as tendon pain. Symptoms It is important to know that pain at the back of the heel is not always due to Achilles tendon rupture. It may be due to bursitis (fluid accumulation in the heel due to repeated irritation) and tendonitis (pain along the Achilles tendon due to constant friction and irritation). The above disorders tend to improve with use of pain medications and rest, whereas Achilles tendon rupture requires surgery and/or a cast. Diagnosis If an Achilles tendon rupture is suspected, it is important to consult a doctor straight away so that an accurate diagnosis can be made and appropriate treatment recommended. Until a doctor can be consulted it is important to let the foot hang down with the toes pointed to the ground. This prevents the ends of the ruptured tendon pulling any farther apart. The doctor will take a full medical history, including any previous Achilles tendon injuries and what activity was being undertaken at the time the present injury occurred. The doctor will also conduct a physical examination and will check for swelling, tenderness and range of movement in the lower leg and foot. A noticeable gap may be able to be felt in the tendon at the site of the rupture. This is most obvious just after the rupture has occurred and swelling will eventually make this gap difficult to feel. One test commonly used to confirm an Achilles tendon rupture is the Thomson test. For this test the patient lies face down on an examination table. The doctor then squeezes the calf muscles; an action that would normally cause the foot to point like a ballerina (plantar flexion). When a partial rupture has occurred the foot's ability to point may be decreased. When a complete rupture has occurred, the foot may not point at all. Ultrasound scanning of the Achilles tendon may also be recommended in order to assist with the diagnosis. Non Surgical Treatment Pain medicines can help decrease pain and swelling. A cast may be needed for 2 months or more. Your foot will be positioned in the cast with your toes pointing slightly down. Your caregiver will change your cast and your foot position several times while the tendon heals. Do not move or put weight on your foot until your caregiver tells you it is okay. A leg brace or splint may be needed to help keep your foot from moving while your tendon heals. Heel lifts are wedges put into your shoe or cast. Heel lifts help decrease pressure and keep your foot in the best position for your tendon to heal. Surgery may be needed if other treatments do not work. The edges of your tendon may need to be stitched back together. You may need a graft to patch the tear. A graft is a piece of another tendon or artificial material.  Surgical Treatment An Achilles tendon rupture is a complete tear of the fibrous tissue that connects the heel to the calf muscle. This is often caused by a sudden movement that overextends the tendon and usually occurs while running or playing sports such as basketball or racquetball. Achilles tendon rupture can affect anyone, but occurs most often in middle-aged men.
Overview
Originally known as posterior tibial tendon dysfunction or insufficiency, adult-acquired flatfoot deformity encompasses a wide range of deformities. These deformities vary in location, severity, and rate of progression. Establishing a diagnosis as early as possible is one of the most important factors in treatment. Prompt early, aggressive nonsurgical management is important. A patient in whom such treatment fails should strongly consider surgical correction to avoid worsening of the deformity. In all four stages of deformity, the goal of surgery is to achieve proper alignment and maintain as much flexibility as possible in the foot and ankle complex. However, controversy remains as to how to manage flexible deformities, especially those that are severe.  Causes Overuse of the posterior tibial tendon is often the cause of PTTD. In fact, the symptoms usually occur after activities that involve the tendon, such as running, walking, hiking, or climbing stairs. Symptoms As different types of flatfoot have different causes, the associated symptoms can be different for different people. Some generalized symptoms are listed. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running and jumping, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time and may experience pain at the inside of the ankle and in the arch of the foot. Feeling like one is ?dragging their foot.? When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain in the bones and tendons in the outside of the ankle joint. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoe wear very difficult. Sometimes, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetic patients may not experience pain if they have damage to their nerves. They may only notice swelling or a large bump on the bottom of the foot. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoe wear is not used. Diagnosis The diagnosis of tibialis posterior dysfunction is essentially clinical. However, plain radiographs of the foot and ankle are useful for assessing the degree of deformity and to confirm the presence or absence of degenerative changes in the subtalar and ankle articulations. The radiographs are also useful to exclude other causes of an acquired flatfoot deformity. The most useful radiographs are bilateral anteroposterior and lateral radiographs of the foot and a mortise (true anteroposterior) view of the ankle. All radiographs should be done with the patient standing. In most cases we see no role for magnetic resonance imaging or ultrasonography, as the diagnosis can be made clinically. Non surgical Treatment Patients can be treated non-surgically with in-shoe devices and braces to hold their feet in the correct position. This can reduce pain and damage and assist with walking. Physical therapy is also given to improve muscle strength and help prevent injury to the foot. Surgery can be performed if the patient doesn?t find any relief. 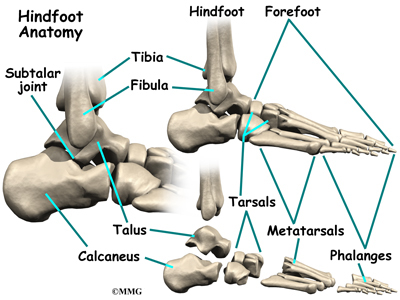 Surgical Treatment If conservative treatment fails surgical intervention is offered. For a Stage 1 deformity a posterior tibial tendon tenosynovectomy (debridement of the tendon) or primary repair may be indicated. For Stage 2 a combination of Achilles lengthening with bone cuts, calcaneal osteotomies, and tendon transfers is common. Stage 2 flexible PTTD is the most common stage patients present with for treatment. In Stage 3 or 4 PTTD isolated fusions, locking two or more joints together, maybe indicated. All treatment is dependent on the stage and severity at presentation with the goals and activity levels of the patient in mind. Treatment is customized to the individual patient needs. |
